
6A: Assessment
This section covers:
What is a pressure injury?
A pressure injury is an injury to the skin and/or underlying tissue, usually over a bony prominence. It occurs as a result of pressure alone, or pressure in combination with shear and/or friction.
Shearing forces usually occur as a result of sliding or dragging the skin across a support surface such as a mattress.
Friction is the abrasion of the epithelial surface of the skin by rubbing against an abrasive or resistant surface. Friction may occur if the client repeatedly rubs their heels on their mattress or wheelchair foot plates.
The presence of constant moisture from perspiration, urinary and/or faecal incontinence or wound leakage affects the ability of the skin to resist this type of damage.
Pressure injuries can occur in any location but are most commonly found on the sacrum (base of the spine) or coccyx (tailbone) and heels. They may also occur on other bony prominences, including the buttocks (ischium), toes, elbows, ears, ankles, nose or other areas such as in the photograph below.
IMAGE - M6 01 Pressure injury on collar boneRisk factors
All clients are at risk of developing a pressure injury, especially those with one or more of the following risk factors.
| Risk factor | Explanation |
| Alteration in mobility or physical activity | Reduced mobility or physical activity due to contractures, fractures, injury, neurological disease or pain increase the risk of pressure injuries developing. This is because the client is unable to independently reposition themselves to off-load or relieve pressure. |
| Malnutrition and dehydration | Malnutrition and dehydration increase the risk of pressure injuries. The skin is much drier and less able to withstand the effects of pressure damage. |
| Moisture | The presence of constant moisture from wound leakage, urinary or faecal incontinence and perspiration increases the risk of pressure damage. This is because the skin is less able to resist friction or shearing forces. |
| Alteration in sensation and consciousness | Decreased sensation or loss of consciousness because of cognitive impairment, such as a central nervous system injury, a cerebrovascular accident, degeneration, major surgery, spinal cord injury or medications, increases the risk of pressure damage. This is because the client may not be aware that an injury to the skin has occurred. |
| Other health conditions | Health conditions such as heart disease, diabetes, circulation disorders and a history of smoking can increase the risk of pressure injury. |
Top of page
Stages of pressure injuries
Pressure injuries are staged or categorised to help you determine how severe the damage to the skin and underlying tissue structures might be. There are four stages or categories of pressure injuries. The higher the stage or category, the deeper is the tissue involvement. These are described further in the following table.
| Pressure Injury Stage | Explanation |
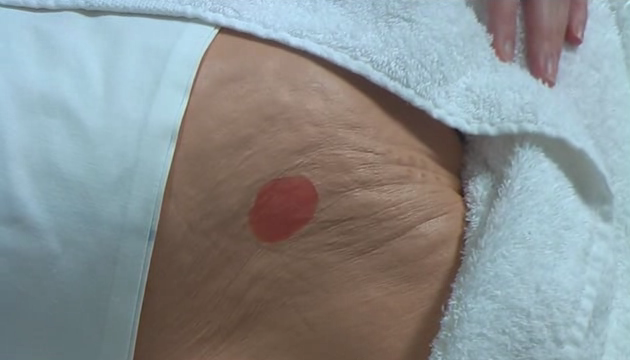
| Stage 1 | Stage 1 pressure injuries present as areas of persistent, non-blanchable redness when compared to the surrounding skin. The skin around the wound may be painful, firm, soft, or warmer or cooler to touch when compared to the surrounding skin. Stage 1 pressure injuries may be difficult to detect in individuals with dark skin tones. In lighter skin toned individuals, if you press on the skin for a few seconds, normal skin typically goes white in colour and then returns to a normal pink colour when the pressure is released. However, clients with darker pigmented skin may not have visible blanching and skin colour may differ from the surrounding area. This means that when you press on the skin, changes in skin colour are difficult to detect. |
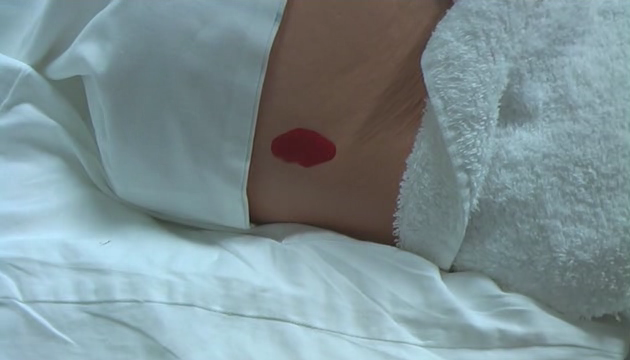
| Stage 2 | Stage 2 pressure injuries represent partial thickness loss of the dermis and present as shallow open ulcers with a red or pink wound bed. They may also present as an intact or open/ruptured fluid filled blister. If a blister is found with clear fluid present and the epidermis is clearly separated from the dermis, this is recorded as a Stage 2 pressure injury. Stage 2 pressure injuries present as shiny or dry shallow injuries without any bruising present since bruising represents suspected deep tissue damage. |
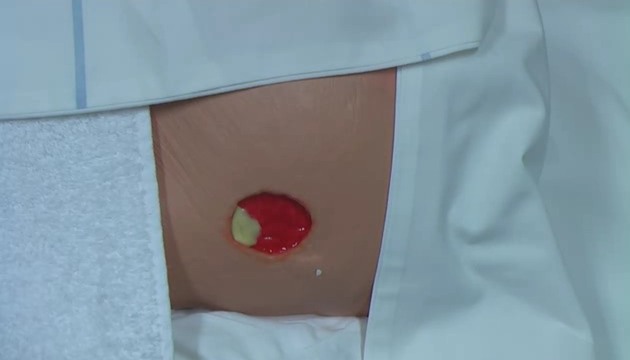
| Stage 3 | Stage 3 pressure injuries represent full thickness skin loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Thick yellow tissue (slough) may be present but this does not obscure the depth of tissue loss. There may be undermining and tunnelling of the wound (i.e. the wound is deeper than it appears on the surface of the skin). The depth of a Stage 3 pressure injury varies depending on where it is located anatomically ( i.e. a pressure injuries on the bridge of the nose, ear, scalp and ankles does not have subcutaneous tissue) and Stage 3 pressure injuries can be shallow. In contrast, areas of significant adiposity or fatty tissue can develop extremely deep Stage 3 pressure injuries but bone and/or tendon is not visible or directly palpable. |
| Stage 4 | Stage 4 pressure injuries are the most severe and represent full thickness tissue loss with exposed bone, tendon or muscle. Thick yellow tissue (slough) or black necrotic tissue may be present on some parts of the wound bed. Often there is undermining and tunnelling of the adjacent tissue. The depth of a Stage 4 pressure injury varies by anatomical location. The bridge of the nose, ear, scalp and ankles do not have subcutaneous tissue so these ulcers can be shallow. Stage 4 pressure injuries can extend into muscle and/or supporting structures (e.g. fascia, tendon or joint capsule) making osteomyelitis (infection in the bone) possible. Exposed bone/tendon is visible or directly palpable. |
In addition to the above stages or categories of pressure injuries there are two other categories of tissue damage, which are explained below.
| Stage | Explanation |
| Suspected deep tissue injury | Suspected deep tissue injury presents as purple or maroon discoloured intact skin or a blood-filled blister due to damage of the underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, or warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. The tissue injury may develop into a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Changes may develop rapidly exposing additional layers of tissue even with optimal treatment. |
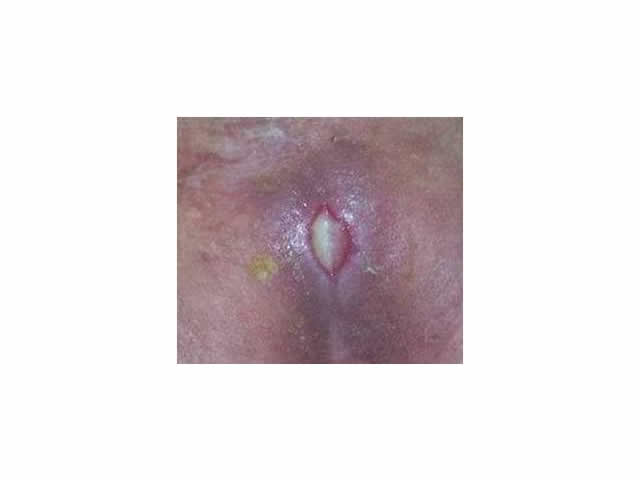
| Unstageable | Unstageable pressure injuries present as full thickness tissue loss in which the base of the injury is covered by thick yellow, tan, grey, green or brown tissue and/or eschar (tan, brown or black) in the wound bed.
Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore stage, cannot be determined. Stable (i.e. dry, adherent, intact without erythema/redness) eschar on the heels serves as "the body's natural (biological) cover" and should not be removed.
IMAGE - M6 07 Unstageable
|
Top of page

M6 01 Pressure ulcer on collar bone

M6 02 Stage 1 pressure ulcer
M6 V01 Staging Stage 1
M6 03 Stage 2 pressure ulcer
M6 V02 Staging Stage 2

M6 04 Stage 3 pressure ulcer
M6 V03 Staging Stage 3

M6 05 Stage 4 pressure ulcer
M6 V04 Staging Stage 4

M6 06 Suspected deep tissue injury

M6 07 Unstageable

M6 V05 Staging Unstageable

